
Cardiovascular Clinical Guideline
Arterial Stiffening
Optimal treatment of high blood pressure and its complications should consider arterial stiffness, central aortic blood pressure and left ventricular wasted energy – all of which should be reduced to the lowest possible level. Preference should be given to vasodilator drugs that affect peripheral muscular arteries, reduce wave reflection amplitude and markedly lower systolic and pulse pressure as well as ventricular after load (Davies and Struthers, 2003, Naschitz and Lenger, 2008).
PWV
The European Society of Hypertension/European Society of Cardiology guidelines have recommended measurement of Pulse Wave Velocity (PWV) as a gold standard for routine evaluation of aortic stiffness in individual patients, clinical studies and for the assessment of target organ damage in the management of hypertension (Mancia et al., 2007, Williams B, 2018).
AI
Arterial stiffness, expressed as Augmentation Index (AI), characterised by increased values of carotid-femoral PWV, has been recognised as an independent predictor of future cardiovascular events and mortality in addition to the known classical risk factors, even in healthy subjects.(Zoungas and Asmar, 2007, Vlachopoulos et al., 2010). AIxis referred to augmentation index at the aorta and AIis augmentation index as measured in peripheral arteries.
Relevance: End-organ damage
The high risk of cardiovascular disease in subjects with chronic kidney disease (CKD) and end stage renal disease (ESRD) can be partially attributed to a stronger presence of other cardiovascular risk factors such as high blood pressure, high cholesterol, diabetes and low activity levels. However, these factors alone do not completely explain the high mortality rates among ESRD patients.
Currently, the strongest predictor of cardiovascular death in haemodialysis patients is the structure and function of the larger arteries. With increased arterial stiffness comes an increase in central systolic pressure and therefore a greater cardiac workload. The arterial stiffness changes the pressure profile at the heart and in the peripheral arteries, thereby contributing to the development and advancement of conditions such as hypertension, left ventricular (LV) hypertrophy and dysfunction and myocardial perfusion.
Arteriosclerosis and increased arterial stiffness (2018 EU hypertension guidelines)
Large artery stiffening is a major factor contributing to the rise in Systolic BP and fall in Diastolic BP with ageing. Arterial stiffness is usually measured in studies as PWV. Arterial stiffening results from arteriosclerotic structural changes in large conduit arteries, leading to a loss of arterial elasticity, and the distending force resulting from the pressure exerted on the arterial wall. Thus, all antihypertensive drugs, by reducing BP, reduce arterial stiffness, as the reduction in BP unloads the stiff components of the arterial wall, leading to a passive decrease in PWV.
Effect of reflected wave (AI%) on forward wave (brachial artery)
Fig 1.

The pulse wave explained: A “normal” pulse wave with “normal” flexibility in the arterial walls will display a systolic peak, Dicrotic notch (aortic valve closes) and diastolic level (more or less even throughout the body).
An increase in arterial stiffness causes the reflected wave (See fig 2.), to extend sideways to accommodate backwards pressure. The pump time is extended (using more oxygen), while the myocardial perfusion time of the left ventricular muscle with oxygen-rich blood is shortened, effectively tiring the heart muscle.
A large increase in arterial stiffness causes an increase in left ventricular load Fig 3, 4 plus the extended pump time, therefore increasing the tiring effect on the heart muscle, leading to increased ventricular mass and an eventual CV event.
Reflected wave generated by arterial bifurcation
Fig 2.
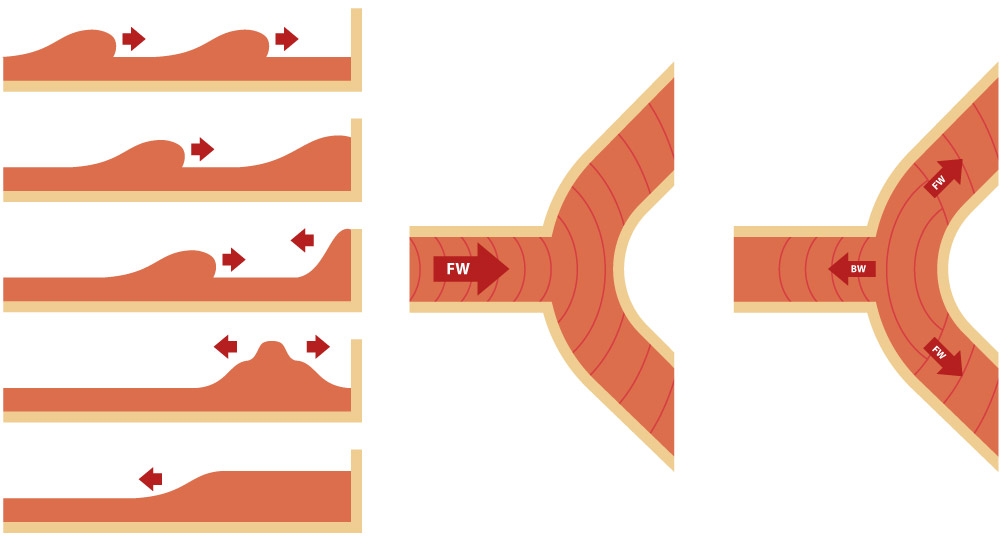
Ascending aorta
Pressure wave recorded in the ascending aorta in a subject with undamaged viscoelastic properties of the arterial wall. The encounter between backward and forward waves occurs at the end of the systole, and the superimposition of the two waves lasts the whole diastole.
Fig 3.

Peripheral artery
Pressure waveform recorded in peripheral artery in a subject with marked arterial stiffness. Early superimposition of backward waves onto a forward pressure wave already characterized by an increase in systolic blood pressure values and by a decrease in diastolic blood pressure values.
Fig 4.

Aortic pulse wave velocity (PWV) and more significantly Augmentation Index (Alx) are known predictors of morbidity in ESRD patients on haemodialysis. These values provide information into mortality and risk independent of other known risk factors. In a patient study group of ESRD subject, an increase of 10 in Alx (%) produced a 5% increase in the risk of cardiovascular and all-cause mortality. In addition, any increase of PWV of 1 m/s showed a subsequent 39% increase in adjusted overall mortality. The characteristics of this patient group included ranges for Alx of 26 ±15 and PWV of 11.7 ±3.0 m/s. All of these findings were independent of other known risk factors including brachial BP.
Pulse wave velocity
Large artery stiffening is the most important pathophysiological determinant of isolated systolic hypertension and age-dependent increase in pulse pressure. Carotid-femoral pulse wave velocity (PWV) is the gold standard for measuring large artery stiffness. It is the rate at which the pulse pressure waves travel down the vessels.
Reference values for PWV are available in healthy populations and patients at increased CV risk. A PWV >10 m/s is considered a conservative estimate of significant alterations of aortic function in middle-aged hypertensive patients. The additive value of PWV above and beyond traditional risk factors, including SCORE and the Framingham risk score, has been suggested by several studies. (2018 ESC/ESH Guidelines for the management of arterial hypertension)
Determining pulse wave velocity requires clinic-based equipment with the patient in a reclined position. The distance between femoral-placed and carotid-placed cuffs is measured, and the pulse wave velocity is calculated. This procedure is not suited for the pharmacy consultation room. Arterial stiffness is reflected in the augmentation index (AI%) value with the BP+. Arterial stiffness is associated with pulse wave velocity, hence the correlative mention in discussions.
Studies show that arterial stiffness in ESRD has widely attributed to vascular calcification. A link has also been found between the presence of vascular calcification and increased arterial stiffness in dialysis patients. Additionally, as the aortic PWV increases, so too does the degree of coronary artery calcification. This finding is significant because calcifications may be a preventable factor in the development of arteriosclerosis in ESRD patients.
Recently, studies have also shown that children on dialysis exhibit major abnormalities in arterial walls and consequently, stiffened large arteries. This finding is shown by increases in Alx and PWV, demonstrating the importance of using these markers in paediatric nephrology to assess and monitor cardiovascular risk.
While increased aortic stiffness (PWV) and systemic arterial stiffness (aortic Augmentation Index - Alx) have readily been shown to correlate with other conditions prevalent in patients with CKD, hypertension, diabetes, atherosclerosis and hypercholesterolaemia there is less documentation linking arterial stiffness to high rates of cardiovascular death in CKD patients. Recent studies do indicate that arterial stiffness is associated to pre-dialysis CKD patients with mild renal impairment. As well, it has been shown that increased arterial stiffness is associated to the decrease in renal function as evidenced by decreasing glomerular filtration rate.
Increasingly, studies are demonstrating the effects of various factors such as drugs, salt and water overload, kidney transplantation and exercise on arterial stiffness in renal and hypertensive patients. In fact, the PWV System has recently been used to analyse the effect of dialysis on endothelial function in renal patients. These applications and linkages highlight the potential of PWV (and AI) to illustrate the effects of therapies and regimens through central blood pressure, changes to the aortic and systemic arterial stiffness, as well as endothelial function changes.
Arterial stiffness and cardiovascular risk
Arterial stiffness and accelerated wave reflections that lead to increased central pressure have been linked to many of the other common cardiovascular illness risk factors such as high blood pressure and obesity. More importantly, studies show that central systolic pressure and arterial stiffness are predictors of cardiovascular morbidity and mortality independent of the usual risk factor or other contributors such as brachial systolic blood pressure.
The measures of systemic and aortic stiffness generated by the BP+ system (i.e. peripheral augmentation index) have been linked to conditions with a high incidence of cardiovascular risk. These parameters have also been independently associated to all-cause and cardiovascular mortality in subjects with end-stage renal failure. In hypertensive and diabetic patients, Al and PWA have also been shown to be significant predictors of coronary artery disease and cardiovascular morbidity/mortality.
Research shows that arterial stiffness produces a rise in myocardial demand and central systolic pressure coupled with a fall in coronary artery perfusion pressure. This physiological occurrence drastically increases the risk of heart attack, stroke and heart failure.
Factors associated with arterial stiffness
Age, Height and Gender
It is widely recognized that age is an important determinant of cardiovascular events. As arteries age, they become increasingly stiff and dilated. This structural change causes an increase in systolic blood pressure and pulse pressure which may eventually lead to hypertension, specifically isolated systolic hypertension (the most common form in the senior citizens).
Studies show a positive correlation between arterial stiffness (Al) and age. This relationship also exists for central pressure pulse (PP) and augmentation pressure (AP), however, Al exhibits a different pattern than the former. Central PP and augmented pressure (AP) increase linearly with age while changes to Al are more prominent in people below age 50 and changes in AI are more significant in people over age 50. Since an increase in arterial stiffness leads to an increase in augmentation pressure and systolic pressure, it is recommended that AI% and pulse wave analysis (PWA) are considered to fully assess the impact of age on arterial health.
Height is said to play a role in the risk for developing cardiovascular disease. In individuals of short stature, there is a shorted path length for pressure waves to travel and the reflected waves arrive back earlier in the cardiac cycle. This causes an increase in systolic pressure and LV afterload.
Women tend to have a higher level of arterial stiffness than men. Some studies suggest that height is the underlying cause of this gender difference as women are typically shorted in stature than their male counterparts. However, even when correcting for this height factor, gender still plays a role in predicting arterial stiffness.
Cigarette Smoking
Smoking has an immediate effect on central blood pressure, endothelial function and vasoconstriction. As such, cigarette smoking is a significant risk factor in the development of cardiovascular disease, even among young people. Regardless of gender, height, health or fitness levels, Alx readings are dramatically higher in smokers. Even occasional smokers exhibit these higher-than-average results with studies showing that secondhand smoke has only a slightly less detrimental effect on arterial stiffness as chronic smoking.
Important to note is that despite the significantly high Alx readings, brachial BP measures tend to be low in chronic smokers due to poor pressure amplification, giving an inaccurate picture of overall health. The PWA System provides a wider view and deeper insight into aortic pressures and arterial stiffness.
Obesity
The rate and prevalence of obesity among children and adults is rapidly becoming a global issue. Over 60% of adults in United States are overweight and the number of children and adolescents who are obese is quickly rising. The linkages between obesity and cardiovascular disease are well established in addition to the association with other conditions such as diabetes, hypertension and sleep apnea. Recently, obesity has also been linked to arterial stiffness with central adiposity being a significant factor in Alx. This relationship is independent of other health factors like age or blood pressure. It now recommended that body fat distribution, as opposed to body weight, be considered when analyzing arterial stiffness.
In addition to arterial stiffness, a relationship between obesity and aortic PWV has been shown to exist. A recent report showed median aortic PWV readings that were 4 to 9 m/s higher in the obese than those within a normal weight range. In addition, the PWV has shown an independent relationship between obesity endothelial dysfunction. After weight loss, significant improvements to vascular endothelial function were observed.
The primary lifestyle change prescribed to obese patients is an increase in exercise. Physical activity has been shown to decrease arterial stiffness both in sedentary subjects as well as in those suffering from coronary artery disease or end stage renal failure. The effect of exercise is far-reaching. It improves arterial stiffness thereby reducing the potential for myocardial ischemia. In addition, exercise shows the potential to alter the natural progression of age-related arterial stiffening. Studies of athletes indicate a lower arterial stiffness than their sedentary counterparts. This difference has been attributed to regular exercise.
Cholesterol
A relationship between high blood cholesterol levels, high central pulse pressures and systemic arterial and aortic stiffness has been shown to exist. This association is significant even despite a low peripheral blood pressure. In addition to this link, LDL cholesterol is an independent determinant of arterial stiffness (shown by a rise in Alx).
It has been determined that lowering cholesterol levels causes a reduction in arterial stiffness as well as a drop in cardiovascular and all-cause mortality. Statin drugs are prescribed to reduce aortic PWV and pulse wave analysis is currently being used in a sub-study of the SEARCH (Study of the Effectiveness of Additional Reductions in Cholesterol and Homocysteine) trial to determine if there are benefits to arterial stiffness in addition to the known benefits to lipid lowering.
Diet
A healthy diet goes hand in hand with good health however, understanding the physiological effect of ingested substances is key. Several foods and drinks influence the cardiovascular system and promote arterial stiffness or lead to cardiovascular risk. The following dietary items have demonstrated a significant effect on the arterial stiffness and central blood pressure.
Caffeine
Caffeine is the most widely used and socially accepted pharmacological substance in the world. Studies show that ingesting coffee produces an increase in central blood pressure while drinking decaffeinated coffee has no effect, thus, caffeine is the active ingredient. An immediate and significant association exists between central systolic pressure, AP, Alx and coffee consumption, without any increase in brachial blood pressure.
In hypertensive patients, this detrimental effect of caffeine is worsened, producing aortic stiffness that lasts up to 3 hours long. For patients that already exhibit a stiffened aorta, this effect is further exacerbated by caffeine with little to no protection coming from anti-hypertensive medication.
Caffeine use produces a detrimental effect on arterial stiffness and, as a result, on left ventricular load. In addition to the known effects of caffeine, when combined with smoking, it produces a synergistic effect on arterial stiffness. For these reasons, it has been suggested that caffeine intake be taken into account when assessing cardiovascular risk.
Alcohol
The relationship between alcohol consumption and cardiovascular risk is ‘U’-shaped: heavy drinkers and nondrinkers are at the high end of the risk while moderate drinkers are in the middle, with lower risk. This same relationship exists between alcohol consumption and arterial stiffness. For example, moderate consumption of red wine in patients with coronary heart disease produces favorable effects to central systolic pressures and wave reflections with no changes to brachial blood pressure. Interesting to note is that a similar result was observed with non-alcoholic red wine. The study, therefore, demonstrates the necessity of measuring central pressuresas compared to conventional blood pressure while assessing the risk potential of various substances.
Dark Chocolate
Dark chocolate contains antioxidants called flavonoids that reportedly benefit the cardiovascular system. Incorporating foods high in flavonoids is recommended in order to decrease arterial stiffness and wave reflections (Alx). Dark chocolate has also been found to exert a positive effect on endothelial function. These benefits suggest an overall positive influence of dark chocolate on the cardiovascular system.
Arterial stiffness and pregnancy
Pregnancy produces a host of physical changes in a woman’s body including changes to the cardiovascular system. It is not uncommon to develop hypertension while pregnant, but the condition can lead to major complication for mother and child if eclampsia develops.
Hypertension during pregnancy can take two forms:
Chronic: Onset of this type of hypertension takes place before the pregnancy or 20 weeks prior to gestation and may develop into eclampsia.
Post pregnancy: This type of hypertension develops 20 weeks after gestation and can develop into proteinuria, multi-organ dysfunction (preeclampsia) and seizures (eclampsia).
If the pregnant patient has pre-existing hypertension, this doubles the risk of developing preeclampsia as well as other issues such as placental abruption and growth restriction. Severe cases of hypertension increase the risk of preeclampsia by 46% as well as leading to an increased potential for maternal and fetal complications.
Prevalence and Survival
Studies suggest that over 50, 000 women worldwide die each year from preeclampsia and maternal morbidity due to permanent CNS damage from recurrent seizures or intracranial bleeds and renal insufficiency. About 5% of pregnancies in the U.S. and U.K. are complicated by preeclampsia and of this 5%, 1 to 2% develop eclampsia. The rate of preeclampsia is further increased in women of low socioeconomic status, extremes in age and women experiencing their first pregnancy. The risks to the fetus include premature birth, placental infarcts, intrauterine growth retardation, abrupted placenta, and fetal hypoxia.
While preeclampsia cannot be prevented, mortality can be avoided with early diagnosis, monitoring and treatment. Hypertension is a significant predictor in preeclampsia and assessing this condition in pregnant women could lead to early diagnosis. A recent study showed that over the over 250,000 women studies, those with gestational hypertension were at a 30% greater risk of developing preeclampsia and those with existing preeclampsia showed a staggering 400% higher risk of death or major morbidity compared to those without hypertension. In addition to these pregnancy concerns, the babies of women with hypertension are more likely suffer adverse effects than babies of women without hypertension.
Currently, brachial blood pressure is the standard measure by which pregnant women are assessed throughout the pregnancy. This type of measure is not sensitive enough to differentiate between the various types of hypertension nor is it able to identify patients at risk of developing preeclampsia. Clearly, the need to identify at-risk patients and distinguish between hypertensive disorders is crucial to managing these issues and improving the prognosis for both mother and child.
Arterial Stiffening and pregnancy
Studies show that arterial stiffness is a primary cause of hypertension. Recently, researchers have been looking into the relationship between arterial stiffness and cardiovascular complications in pregnant women. The typical cardiovascular response to pregnancy in a healthy female is an increased heart rate, lowered brachial blood pressure (due to the dilation of peripheral blood vessels), the expansion of blood volume and a rise in endothelial nitric oxide release. Additionally, aortic Alx is typically lower during each of the trimesters as compared to nonpregnant women.
Arterial stiffness causes a premature return of the reflected pressure wave in arteries. Observing the pulse wave analysis provides an important insight whether or not the changes exhibited in aortic Alx are normal or a cause for concern.
Women with gestational hypertension tend to have higher aortic Alx values in their third trimester than non-hypertensive, pregnant women and these values increase in women with preeclampsia. Six weeks after giving birth, the aortic Alx values drop to normal, non-pregnant levels. By the same token, research suggests that aortic stiffness is higher in the presence of gestational hypertension and preeclampsia. As such, the readings for Alx and aortic PWV provided by the PWV System are important for establishing a distinction between women with gestational hypertension and those at risk for progressing to preeclampsia.
Diabetes Mellitus
With heart disease being the number one cause of death among adults, it is crucial to manage factors that contribute to its onset. Diabetes and, in particular Type 2 diabetes, increases the risk of heart disease and stroke due to their associate risk factors such as high blood pressure and high cholesterol. The long-term complications of diabetes are far-reaching and affect many parts of the body. These issues include nerve damage, blindness, kidney failure, stroke and heart and vessel disease. Early identification and symptom management of macrovascular disease are essential for diabetic patients. The BP+ System helps to assess risk and helps to track the progress of cardiovascular complications in a noninvasive, easy-to-use application.
Prevalence and Survival
Diabetes is said to affect over 20 million people in the United States alone. Of this 20 million, 14 million have been diagnosed and another 6 million are living with the disease but have yet to be diagnosed. Around 1 million people over the age of 20 are diagnosed with diabetes each year. The survival rate for diabetics who develop heart disease is 40% and this risk is 2-7 times higher in those patients with Type 2 diabetes. The linkage between diabetes and cardiovascular disease is well documented. In addition, diabetes has been shown to be among the primary causes of end stage renal disease, a condition that also leads to cardiovascular disease.
Arterial stiffness
The relationship between diabetes and a higher risk of cardiovascular events may be, in part, attributed to the other known risk factors (i.e. hypertension, dyslipidaemia, hyperglycaemia and obesity) associated with diabetes. That said, these factors cannot completely account for the link because some of the increased risk is independent of these issues and varies depending on the type of diabetes.
What is clear is that increased arterial stiffness is associated to both Type 1 and Type 2 diabetes and may also contribute to the high mortality rates. The BP+ System provides insight into arterial stiffness which presents a valuable tool for assessing cardiovascular risk in diabetics. The parameters measured by the BP+ System include peripheral pulse pressure and arterial stiffness.
Peripheral pulse pressure assists in the assessment of arterial stiffness and has been shown to correlate to diabetes. Studies show that age-related blood pressure increases progress 15-20 years in Type 1 diabetes. This finding suggests accelerated vascular aging, a precursor to cardiovascular illness.
Augmentation Index, as collected by the BP+ System, indicates arterial stiffness and is an independent predictor of mortality in diabetic subjects. The increased arterial stiffness and augmentation index (pAl) are associated to both types of diabetes.
A recent assessment in the FIELD (Fenofibrate Intervention and Event Lowering in Diabetes) Study illustrated a clear linkage between augmentation pressure (AP), Al and carotid intima-media thickness (IMT) (a known predictor of atherosclerosis in Type 2 diabetes patients). This finding suggests that arterial stiffness may play a role in the advancement of atherosclerosis in Type 2 diabetics. More significantly, this finding suggests that an assessment of central blood pressure and arterial stiffness offer superior potential as determinants of arterial thickening in Type 2 diabetics versus traditional methods. Research into AP and Al is ongoing and expected to provide further insight into the predictive value of these measures as they relate to cardiovascular events in diabetics.
AP and Al are also significantly associated to carotid IMT and plaque score patients suffering diabetes as well as coronary artery disease. In addition, the CURES (Chennai Urban Rural Epidemiology Study) study, as conducted on Asian Indians, (a subsection of south Indians at high risk for developing diabetes and coronary artery disease) demonstrated higher Al and IMT values for Type 2 diabetes patients with retinopathy as compared to those without. This recent finding suggests a strong correlation between early atherosclerosis and diabetic retinopathy.
The BP+ System also offers great potential for assessing risk and optimising treatment in diabetic children. When compared to non-diabetic children, subjects as young as 10 years old with Type 1 diabetes exhibited increased arterial stiffness (Al). The information regarding arterial stiffness as gleaned from the BP+ System may be used to assess risk, improve therapy and manage complications that may arise later in life
Increase arterial stiffness is known to produce an increase in central systolic pressure which, in turn, raises the myocardial demand. The increase in cardiac workload is directly related to arterial stiffness and may result in further cardiovascular-related conditions such as hypertension, left ventricular dysfunction and a decrease in myocardial perfusion. The development and advancement of conditions like these is avoidable with proper identification and monitoring. The BP+ System uses pulse wave analysis and central systolic measures to assess parameters such as arterial stiffness and Al. The information is gathered in a simple, noninvasive manner and once collection, the data is highly valuable in the assessment of existing conditions and prescription for future therapeutic programs.
Customised drug treatment programs have been shown to decrease arterial stiffness in patients with cardiovascular disease, including diabetics. These timely pharmacological interventions have been shown to be effective independent of changes in cuff blood pressure. While insulin has been observed to decrease Al independent of peripheral vascular resistance, this effect is not present in diabetics (Type 1 or Type 2) or obese patients with insulin resistance. Pharmacological interventions which have proven successful in decreasing arterial stiffness include the oral administration of ascorbic acid over a 4-week period. Using the BP+ System, doctors are able to monitor the efficacy of particular drug regimens by measuring changes in central cardiac parameters. This application assures physician’s a reliable patient risk assessment and accurate measure for tracking treatment and managing patient health.
Peripheral Arterial Disease
What Is Peripheral Arterial Disease?
Arteries may become narrowed due to a build-up of a fatty substance called plaque. As the plaque coating the arterial wall accumulates and hardens, the arterial opening becomes smaller, or occluded. This process is referred to as stenosis. When it occurs in the legs and feet, the condition is called lower extremity peripheral arterial disease and it causes pain, poor healing, and in some cases, tissue death. This disease is one way in which atherosclerosis is experienced among the 35% of Americans who suffer from the condition. Other ways in which atherosclerosis is manifested in patients includes other cardiovascular issues such as heart disease and carotid artery disease.
What Are the Risk Factors and Symptoms for Peripheral Arterial Disease?
The most significant risk factor for developing lower extremity arterial disease is smoking. Smoking is, in fact, the primary risk factor for every cardiovascular disease. Other contributing factors include a family history of atherosclerosis, diabetes, high blood pressure and/or high cholesterol, a sedentary lifestyle, and age.
Symptoms of peripheral arterial disease include the following:
Cramping in the lower leg (i.e. calf or thigh) which may lead to claudication
Numbness, weakness, pain or a cool feeling in the legs and feet while at rest
Slow healing of wounds in the lower extremities
Sores or ulcers that develop when the blood supply is compromised (may become gangrenous if left untreated)
Darkening or black discolouration of the toes or skin near the occluded artery
Physicians determine the location and degree of arterial stenosis using imaging tests such as a magnetic resonance imaging (MRI) or angiography. They measure the severity of stenosis and loss of blood flow by comparing blood pressure reading from the ankle as compared to readings from the arm. This test is referred to as the ankle brachial index (ABI).
What are the Treatments for Peripheral Arterial Disease?
Treatments available to patients with peripheral arterial disease depend upon the severity of their condition. For mild to moderate symptoms, lifestyle changes such as increased exercise or quitting smoking are often enough to improve the condition. Doctors may also prescribe a treatment program of blood-thinning drugs or other medications to assist with related conditions such as high blood pressure, high cholesterol and diabetes.
For more advanced stages of the disease, doctors will prescribe more invasive procedures such as balloon angioplasty or stents to physically improve blood supply and widen the arterial opening. These treatments are administered in cases where the diseased area of the artery is relatively small and easily accessible. While initially effective, blockage return with a year or two in about 30-40% of patients treated with an angioplasty or stenting. This return of blockage is called restenosis.
Angiogram
This diagnostic imaging test gives doctors a window into the state of blood vessels. An angiogram conducted on arteries is called an arteriogram while one conducted on the veins is a venogram. In either case, dye is injected into the vessels using a flexible, hollow tube called a catheter. The catheter administers dye through a needle puncture in the groin area. The dye renders the blood vessels visible by x-ray which enables easy viewing and diagnosis of blockages, clots, enlargements and other abnormalities. The doctor may use an angiogram in combination with any of the following treatments including balloon angioplasty, stenting, atherectomy, cryoplasty, or laser treatment.
Balloon angioplasty
The catheter is tipped with a specialized balloon then inserted into a blood vessel in the groin area. The catheter is guided to the affected area of the artery then the balloon is inflated. The inflation causes the plaque to compress against the arterial wall thereby decreasing the blockage and opening the artery.
Stenting
Depending on the extent of blockage, a more permanent solution may be prescribed. For these situations, a small mesh support tube called a stent will be used to reinforce the arterial opening. The stent is inserted using the balloon-tipped catheter. Following inflation, the stent will remain in the artery to assist with flood flow and maintain the newly-enlarged opening. In some cases, the stent will be coated in medication to prevent the formation of scar tissue.
Atherectomy
An atherectomy is performed in conjunction with an angioplasty to remove plaque lining the arterial wall. The atherectomy device is inserted into the artery using catheter. At the site of the arterial blockage, a rotating blade or burr is activated and begins grinding down hardened plaque from the interior walls. The catheter then suctions the loosened plaque out of the body.
Cryoplasty
A balloon angioplasty is performed to expand the arterial wall. A freezing compound is then used at the blockage site. The freezing action causes the plaque to solidify and shatter in smaller, uniform pieces. This process is said to said to stave off restenosis.
Laser
The catheter is tipped with a specialized laser then inserted into the artery. At the blockage point, the laser emits a pulsating laser beam which vaporizes the plaque.
Leg Bypass
For severe cases of arterial disease, a leg bypass procedure is recommended. The bypass involved reconstructing a new blood vessel in the leg in order to improve blood flow, promote wound healing and relieve any associated pain in the legs or feet.
Effects of Physiological Phenomena on The Arterial Pulse
Growth and Development
The arterial pulse in infants shows the same contour in central and peripheral arteries. This finding is similar to what is observed in the elderly. While the amplitude of infantile arterial pulse is low, it shows no secondary wave in diastole and the wave’s peak is observed in late versus early systole. As subjects grow into adolescence, the contours observed in arterial waves begin to change. The peripheral pulse is amplified, the wave peak shifts to early systole and the secondary diastolic wave is now obvious during early diastole. These changes to the pressure wave contribute to the significantly higher peripheral pulse pressure and systolic pressure experience in late adolescence versus infancy.
The similarity in pressure pulse waveform between infants and the elderly can be attributed arterial structure and its effect on wave reflection. In infants, wave reflection from peripheral to central vessels is short due to their relatively short length of the infant’s body, even though the aorta is very compliant at a young age. In the elderly, body length isn’t the significant factor; however, aortic stiffness produces the same effect on the reflected wave velocity. Despite their short bodies and quick heart rate, infants show a relatively long LV ejection period. During research, animals of similar size and heart rate indicate a significantly shorter LV ejection rate and secondary reflected waves are noticed in diastole versus systole.
This transfer function for producing increasing aortic pressure waves is illustrated in adults rather than children. The shorter body length of younger people affects wave travel and reflection significantly. The pressure pulse waves are affected in the upper body as well as the lower limbs, wherein most reflection originates.
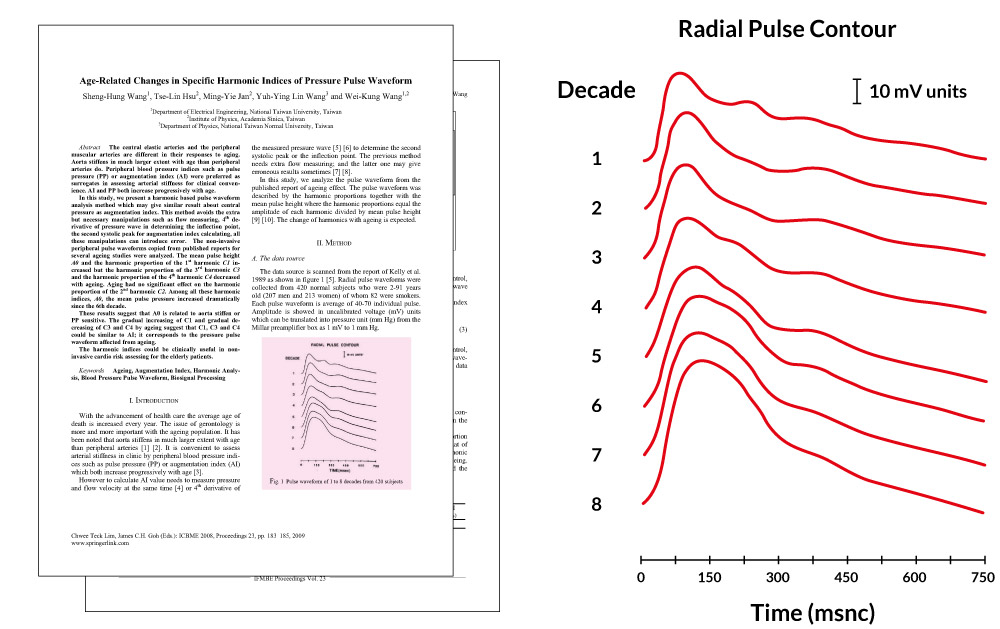
Ageing
Dating back to Mahomed’s initial observations, age has been found to be significant factor in the arterial pulse. Kelly et al. have conducted extensive research on this arterial pulse in normal subjects. Findings show an increase in the late systolic pressure peak in both the radial and carotid arteries. This observation is coupled with the loss of the secondary diastolic pressure wave. In addition, the late systolic pressure wave is found to be lower in the radial artery that in the carotid, regardless of age. Similarly, it has been found that readings from the ascending aorta taken at the cardiac catheterisation show the same pulse wave patterns however, late systolic augmentation is greater in the carotid and even more so in the radial artery.
Augmentation is defined as the boost to late systolic pressure after the first initial systolic shoulder. This reading is determined by dividing pulse pressure by the pressure to the first systolic shoulder and it is expressed in mmHg. It can also be determined by dividing augmentation by pulse pressure. Augmentation of the aortic wave is measured as 20 mmHg or 159% (or 37% of pulse pressure).
Augmentation is said to increase with age. In adolescence, augmentation index is around 50%, with amplitude of the systolic pressure wave approximating the reflected wave. This value increases accordingly with age so that elderly people show an augmentation index of about 80-100%.
This trend in increasing augmentation index throughout life is directly related to arterial stiffening, particularly aortic which increases pulse wave velocity. Arterial stiffening causes an early return of the reflection from the trunk and lower body. This reflection takes place throughout the body wherever low resistance conduit arteries join high resistance arterioles. This action has been researched extensively in normal western versus normal Chinese subjects. The Chinese population has a statistically low occurrence of atherosclerotic disease. It has been shown that aortic wave velocity increases by more than double between the ages of 20 and 100 therefore the process of aortic stiffening is a normal ageing response and responsible for the increases observed in pulse pressure and systolic pressure. The process is exacerbated by hypertension and arterial degeneration and may be modified by arterial and cardiac disease.
Physical Fitness
It appears that the ill effects suffered as a result of ageing on the arterial pulse coupled with the lower systolic augmentation of the pulse in various arteries has a detrimental effect on physical fitness. It has been suggested that exercise affects the overall endothelial functioning in the body, causing conduit arteries to dilate (endothelial nitric oxide dump) , wave reflection to decrease and pulse wave velocity to drop. These effects could produce a decrease in augmentation of the carotid, radial or aortic pulse, however, this relationship has not been established and a dominant mechanism for the observed results has not been determined. It has also been posited that subjects with less aortic ageing may simply feel more comfortable during exercise than those with an advanced condition and therefore are more likely to take part in exercise.
Lower augmentation readings in fit subjects may be attributed to improve endothelial function; however, a relationship between pulse wave contour and endothelial dysfunction has not been established. Changes in pulse wave velocity and instances of arterial stiffness in the upper limbs are not associated to endothelial dysfunction in the upper limb as observed with age in different diseases.
Food
Food consumption of any sort (including drinks) produces a reduction in wave reflection from the splanchnic bed thereby altering the contour of the arterial wave especially the degree of late systolic augmentation. As such, the post absorptive state is preferable for conducting assessments on ageing, drug effects or of the disease in general.
Heart Rate
Both the pattern and duration of ventricular ejection are affected by heart rate. This, in turn, leads to changes in the contour of the arterial pressure wave as well as the summation of reflected waves as produced during ventricular ejection. It has been found as heart rate decreases, augmentation increases (through an increase in the ejection period) and as heart rate increases (and ejection period shortens), augmentation decreases.
Exercise
Exercise produces an obvious effect on heart rate and is most apparent during tachycardia when pulse pressure in the radial artery may increase to twice as much as in the ascending aorta and radial systolic pressure rises to 80 mmHg or higher. The vertical bodily effect of running causes additional pressure waves to show in the arterial pulse though it appears that in trained long-distance runners, a counter pulsation may be experienced wherein heart rate and stride are entrained and the vertical action causes the most significant boost during diastole. If reversed, this phenomenon could have a detrimental effect with diastolic pressure reduced and systolic pressure boosted.
Body Height
Augmentation is highly dependent on height, regardless of age and for every artery. A short stature is a known predictor of cardiovascular disease and differences in height are the primary reason for the variance in augmentation between males and females. Shorter body heights cause an early wave reflection. The resulting increase in aortic systolic pressure augmentation with increased LV load and LV hypertrophy may be the primary mechanism causing the effect.
Gender
Gender-related differences in augmentation are primarily attributed to the differences in height between men and women. Oestrogens do contribute to arterial stiffness and changes in pulse contour however stature is thought to be the major factor.
Effects of Disease on arterial stiffness
Arteriosclerosis
The most significant factor in arterial pulse is ageing. In all human subjects, aortic pulse wave velocity gradually increases with time as does the progressively early return of the reflected wave. This results in the secondary wave in diastole moving into systole with greater augmentation of pressure in late systole. Late systolic pressure augmentation caused by early wave reflection is attributable for a 40±50 mmHg boost to systolic pressure in central arteries.
At the root of aortic stiffening is the fracture and fragmentation of elastic lamellae within the media. Progressive aortic dilation occurs when stresses are transferred from the elastin in arterial walls to less extensible collagen areas, producing an increase in stiffness. The phenomenon causes a disorganization and dilation in the aorta and arteries in regions of ‘medio necrosis’. This generalized degeneration of medial elements in elastic arteries is referred to as arteriosclerosis. This disease produces a progressive increase in pulse pressure and systolic pressure, otherwise known as isolated systolic hypertension.
Hypertension
Systolic hypertension may have the same effect on pressure wave changes as ageing; however the accelerated aortic degeneration would take place at an earlier age. This effect of hypertension is easily explained by increased stiffness and accelerated pulse wave velocity in the aorta. While acute, it is reversible. This change in arterial pulse combined with increased amplitude in the secondary systolic pressure wave in the radial artery was cited by Mahomed as compelling proof of elevated arterial pressure. For over 20 years, Mahomed used this observation in clinical studies until the later Riva-Rocci cuff method took its place.
Atherosclerosis
There are many studies describing increase in arterial stiffness in patients with coronary artery disease or with other evidence of atherosclerosis. Despite this, and despite our every opportunity, we have not been able to gauge the severity of atherosclerosis on the basis of the arterial pressure wave, and we are not aware that others have been able to accomplish this in prospective studies. We have not been able to show any definite difference in aortic pulse wave analysis in patients with generalised atherosclerosis and cannot propose this as a screening test for atherosclerosis. Neither can others who have studied this possibility.
Atherosclerosis must stiffen the aorta and must contribute to early wave reflection. We are surprised that it has so little effect on measured indices of arterial stiffness, or on the contour of the arterial pulse, which is so sensitive to changes in such indices.
Diabetes Mellitus
It has been cited that diabetes increases arterial stiffness, however, neither the measurement of pulse wave contour nor readings of aortic stiffness help to diagnose diabetes mellitus. Similarly, these measurements have not proven helpful in assessing the extent of the disease. Research indicates that an increase in aortic augmentation in diabetic patients (both Type 1 and 2) does correlate to increases in aortic stiffness. However, it appears that ageing and the effects of hypertension are the primary factors leading to aortic stiffness and changes in pulse wave contour in atherosclerosis and diabetes mellitus.
Premature Aortic Degeneration
It is not uncommon to encounter patients with marked aortic augmentation that is higher than normal for their age or arterial pressure level. Typically, these abnormal findings are in middle-aged females in good health but with instances of vascular disease in their family history. Some of the study subjects have exhibited cerebral vascular events before the age of 55, an atypical occurrence. Further investigation into at-risk subjects is necessary to make conclusive statements, however, premature cardiovascular events may eventually prove the earlier claim by Mahomed: “by his pulse you will know him.”
Heart Failure
Pulse wave analysis is particularly useful in the screening process to predict heart failure. During LV dysfunction, it has been recognized that ejection duration is prolonged due to a slower rate of calcium re-uptake. This action is often observed in collaboration with left ventricular hypertrophy. This observation has been used to assist in diagnosing diastolic left ventricular dysfunction in subjects suffering from cardiac failure. It is also useful in distinguishing diastolic LV dysfunction from systolic LV dysfunction.
Ejection duration is lower during systolic LV dysfunction as a result of the premature wave reflection producing a significant effect on pressure flow. This action contributes to the following functions: presence of a dicrotic pulse during systolic heart failure, shortened ejection duration, minimal to no central pressure augmentation and anapparent wave reflection during diastole. This measure is used to distinguish systolic from diastolic dysfunction as well as gauge the severity of the dysfunction. The capacity to increase ejection duration correlates to this severity. Glyceryl trinitrate is used to enhance readings through a reduction in wave reflection, increase in cardio output and LV ejection duration and a decrease in LV load.
Effects of Drugs
The BP+ System provides insight into positive effects of vasodilator drugs through pulse wave analysis. These effects may not be revealed through traditional cuff measures of arterial pressure. For example, a decrease in ascending aortic and LV systolic pressure are the result of a decrease in amplitude of the secondary systolic wave. This phenomenon occurring in the radial artery indicates an anti-anginal drug effect that is partially due to a lowered LV load. The BP+ System reaches similar conclusions using aortic pulse pressure in order to quantify the effects of vasodilators. This method conveniently provides other instances of ventricular vascular interaction and is able to identify the secondary systolic shoulder on the radial pressure wave.
Observations into the effects of vasodilators on the body are explained by changes in wave reflection. It appears that peripheral systolic pressure is maintained regardless of the drop in central aortic and left ventricular systolic pressure following administration of nitroglycerin. This effect suggests that vasodilators produce a more dramatic effect on the heart than previously assumed (based on observations derived from conventional methods). Since the ascending aortic pressure wave during nitroglycerin infusion can be derived from the radial and the brachial transfer function is minimally changed, we can conclude that vasodilation has a more marked effect on the upper limbs versus the lower body.
Synthesized aortic pulse is frequently used to track the therapeutic effects of treatment in angina pectoris, hypertension and cardiac failure. The predominant goal of drug intervention is to optimise ventricular- vascular interaction while decreasing the reflected wave and reducing aortic augmentation, aortic and LV systolic pressure. Vasodilators increase the ejection period by shortening wave reflection, which, in turn, increases stroke volume. As such, ejection duration of the aortic pulse waveform during systolic failure is shortened.
The prolonged rate of ejection duration is observed in the carotid, radial and aortic pulse. How much the ejection duration is prolonged is directly related to the degree of cardiac failure. Aortic flow waveform has been used in Japan as a measure of the detrimental effects produced by early wave reflection as observed in aortic flow. It is also used to demonstrate how vasodilators successfully reduce wave reflection.
In addition, pulse wave analysis shows potential for studying the effect of nitroglycerin on arterioles and peripheral resistance. The efficacy of nitroglycerin is attributed to its method of dilating conduit arteries in order to reduce wave reflections. The present recommended dosages of nitrates combined with sildenafil (Viagra) is of great consideration since these restrictions have been made in the absence of pulse wave analysis. Rather, these recommendations have been made based on a test group whose blood pressure dropped dramatically whenadministered concurrent doses.
Independent studies suggest that sildenafil and nitrates produce a significant reaction when combined. Research indicates that sildenafil potentiates the effect of nitroglycerin by up to twice the intended result and prolongs this effect for as many as 8 hours. The PWV System uses pulse wave analysis to safely track and monitor this drug interaction in order to facilitate titration of nitroglycerin (if required after sildenafil).
The arterial pressure pulse provides insight into potential negative effects of drugs. It indicates that b-adrenoceptor blocking drugs typically produce an increase in ejection duration and wave reflection. While uncommon, in some cases, these drugs may cause an increase in aortic and LV systolic pressure as well as an increase in central augmentation. Typically, the positive effects produced by b-adrenoceptor blocking drugs are the result of a disproportionate increase in diastolic, versus systolic, duration with bradycardia.
Unlike nitrates, calcium channel antagonists reduce aortic systolic pressure augmentation via vasodilation. This desirable effect is offset by their potential to decrease the diastolic period and prolong ejection duration even in the absence of cardiac failure. By reducing coronary perfusion time, this may contribute to angina pectoris, particularly if tachycardia takes place during the same time.
This phenomenon may provide the underlying cause of angina and myocardial ischaemia with short-acting dihydropyridines.
Disclaimer: This reference material is intended for use by qualified healthcare practitioners. The information it contains is presented for general educational use only and is independent from the products itself. While every reasonable effort is made to ensure that the information provided is accurate, no guarantees for the currency or accuracy of information are made. This reference material relating to information (or to third party information, products and services), is provided 'as is’. All Medi-stats results, and analysis should be considered in the context of person's case history, symptoms, diagnosis, current medications, treatment plans and therapies. Final diagnosis is the sole responsibility of the registered medical practitioner after the patient’s examination, lab tests and/or other clinical findings as necessary. Curtesy of: Medeia